|
Lymfe vloeistof: We hebben ongeveer 11 liter
lymfe vloeistof in ons lichaam. Het zit rond alle cellen en de
voedings en afval stoffen gaan hier doorheen van en naar het bloed.
Het voert grote eiwitten en witte bloedlichamen door een eigen
systeem af omdat deze te groot zijn om door de capillaire membraan
te gaan. Daarnaast heeft het nog een aantal functies voor het
immuunsysteem.
Dr Perrin geloofd dat CFS/ME ontstaat door verstopping van het lymfe
drainage systeem. Giftige stoffen blijven in de hersen met name de
hypofyse en het ruggemerg en spieren zitten waardoor oa hormonale
storingen ontstaan. Draineringsmassage veel bewegen, op en neer
springen op een trampoline en supplementen moet helpen om de
vloeistof beter door te laten stromen.
The Perrin Technique™ is based on Dr Perrin's theory that different
stress factors whether physical, allergies, emotional or infections
lead to an overstrain of the sympathetic nervous system.
Further investigation has led to a probable cause of this nervous
system overload being a build up of toxins in the fluid around the
brain and the spinal cord.
Some of the poisons caused by infection or inflammation in the head
or spine flow through perforations in a bony plate (the cribriform
plate) just above the nasal sinuses into the lymph ducts of the face
and neck.
The toxins are also meant to drain down the spinal cord and out into
the lymph ducts lying along the spine. In a CFS/ME
sufferer these normal drainage points are congested.
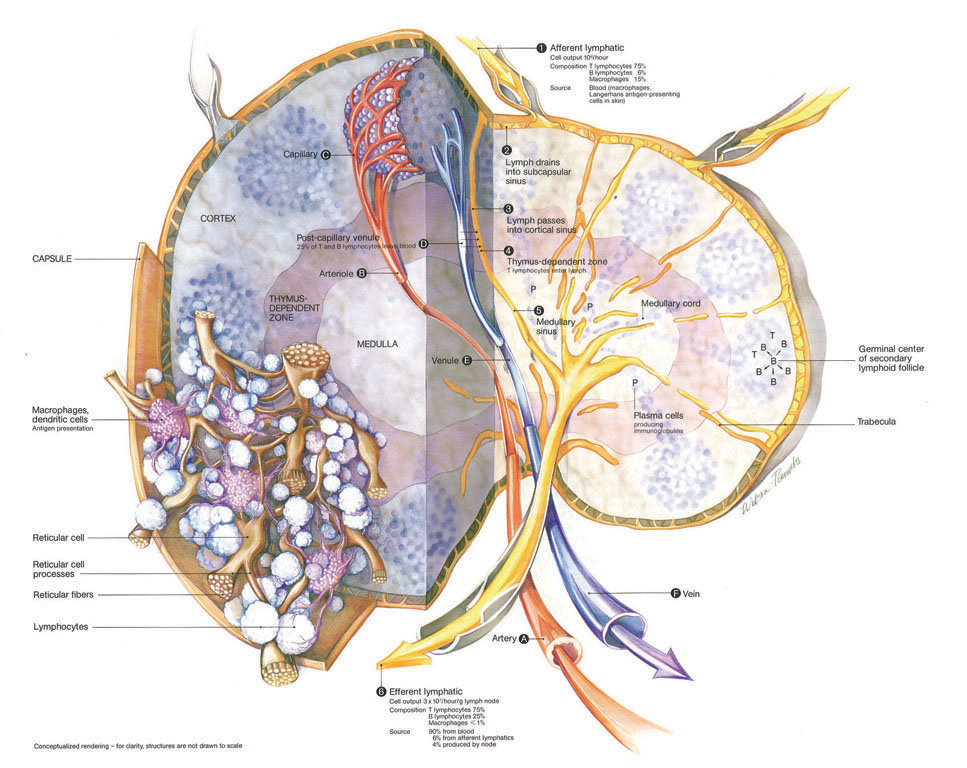
Lymph fluid entering a lymph capillary
It is estimated that your body has more than 100
million different kinds of antibodies, each one
custom-built to identify a particular pathogen. If your
body is exposed a second time, no symptoms occur because
the organism is destroyed quickly- you are now immune to
that particular pathogen.
Oxidative Lymphopathy
Lymphopathy (lymph-au-pathy) is a term for
formation of microscopic clots in lymph, the
pale-white fluid that flows in lymphatic
channels. Like circulating blood, circulating
lymph also clots and unclots at all times. In
CFS, lymph microclots cause blockage of lymph
channels and stagnation of toxic fluid in
tissues. Thus, oxidative lymphopathy adds to
fatigue, muscle pain, brain fog, and other
symptoms of CFS. (Ref: Ali M. Oxidative
regression to primordial cellular ecology. The
Journal of Integrative Medicine 1998;2:4-49.)
.
Water, fruit en groenten voor de drainage.
Drink veel water. Zonder voldoende water kan lymfevocht niet goed
stromen. Als je onvoldoende hoeveelheden water per dag drinkt, zal
uw lymfesysteem vertragen.
De enzymen en zuren in rauwe groenten zijn krachtige lymfe reinigers,
met name wanneer deze gegeten wordt op een lege maag. Voeg meer
rauwe groenten, fruit, salades en verse sappen toe aan uw dieet en
je lymfe zal het instrumenten worden wat je nodig hebt voor een
diepe reiniging.
Flavonoïden, appelzuur, citroenzuur, chininezuur en enzymen in
cranberries en cranberrysap helpen om hardnekkige vet in het
lymfestelsel te emulgeren. Zorg dat je alleen pure, ongezoete
cranberry sap vrij van zoetstoffen drinkt - gepasteuriseerde flessen
cranberrysap hebeben niet dezelfde voordelen. Verdun het sap in een
verhouding van ongeveer 4:1, water /cranberrysap. Als u liever een
minder zure sap heeft, verdun 1 deel ongezoet cranberrysap met 2
delen puur appelsap en 2 delen water. Zorg ervoor dat u alleen puur
appelsap drinkt zonder zoetstoffen of conserveringsmiddelen.
Eet veel groene groenten.Die voorzien u van chlorofyl (de groene
kleur in planten) en tal van vitaminen en mineralen die helpen bij
lymfe reiniging.
Voedingsmiddelen rijk aan essentiële vetzuren zijn essentieel om een
goed functionerend lymfe-systeem te waarborgen. Sommige van deze
voedingsmiddelen zijn lijnzaad en koud geperste lijnzaadolie, verse,
rauwe noten en zaden, zoals walnoten, amandelen, hazelnoten,
zonnebloempitten en pompoenpitten, avocado's en koudgeperste oliën,
zoals walnoot en pompoenpitten. Zorg ervoor dat u verse, rauwe noten
en zaden koopt van het gekoelde gedeelte van uw lokale gezondheids
voedselwinkel of supermarkt. De essentiële vetzuren in noten en
zaden worden snel ranzig.
versnelde pompwerking door te springen
There
is a new medical perspective emerging in the world today: Disease
and aging are intimately related to the acid/alkaline balance (pH)
of the fluids in our bodies. Virtually every degenerative disease
from cancer, osteoporosis, heart disease and arthritis, to skin
problems, tooth decay and joint pain is associated with excess
acidity in the body.
Calcium & mineral absorption is the ultimate
alkalizer
Acid or Alkaline?
We are comprised of approximately 70% water.
Water is comprised of hydrogen and oxygen [H2O]. When there is an
equal proportion of oxygen (O-) and hydrogen (H+), then the pH [potential
hydrogen] is said to be neutral and the pH is 7.0 as measured on the
pH scale that ranges from 1 to 14. If there is more oxygen than
hydrogen the water is alkaline and will measure between 7.1 and 14.
If there is more hydrogen than oxygen the water is acidic and can
range from 1.0 to 6.9 on the pH scale. Most importantly, the pH
scale is logarithmic, which means that each step is ten times the
previous one. Therefore, a pH of 7.0 means that there is ten times
more oxygen available to the cells than a pH of 6.0 and 100 times
more available oxygen than a pH of 5.0. A small variation in pH
measures a rather large difference in the balance between oxygen and
hydrogen.
Everyone knows we need to provide our lungs
with adequate amounts of oxygen to sustain life. We now understand
that the water in our bodies also needs adequate amounts of oxygen
to resist disease and maintain health. The ONLY way to increase the
amount of oxygen in our body “water” is to raise the pH level and
provide the system with the optimum amount of oxygen. MMP Primary &
Trace Minerals can raise your lymph pH to its naturally healthy
level of 7.4 and create an environment for the body to heal itself
and to attain that cherished condition called Super Health.
Now we’re getting somewhere. But how do you
raise the lymph pH? How do you measure it? And what is lymph anyway?
Lymph & pH
To get a sense of how this works, it is important
to understand more about our Lymphatic System. The Lymphatic System
is a complex set of fluids, organs, cells, and lymph nodes
positioned throughout the body forming a circulatory system that
operates in close partnership with blood circulation. This system is
the conduit for the lymph. The word “lymph” in Greek means a pure,
clear stream. When you are Super Healthy, your lymph is indeed a
pure clear stream with a pH of 7.4 flowing through the body quickly
and efficiently, clearing infection, disease and acidic residue. The
cells, organs and tissues of the body are bathed in this oxygen rich,
slightly alkaline lymph fluid creating the BIO-ENVIRONMENT within
which they exist. A 150 pound adult has approximately 22 pounds of
lymph.
Lymph with a pH of 7.4 provides a nurturing,
supportive environment, supplying all the oxygen required for
vibrant heath. Just as we need oxygen available in our external
environment to live, we also require oxygen available in our
internal environment to thrive. Unfortunately, due to diet and the
lack of nutrients in the foods we eat, the average American adult
has a lymph pH of 6.2. Remember the pH scale is logarithmic.
Therefore, a drop in pH from 7.4, which is where we start as
children, to an adult average of 6.2, means there is a 94% decrease
in the amount of available oxygen in the lymph. Imagine living in an
environment that provides only 6% of the oxygen you need. Not a
place where you would want to live. Well, that is exactly the kind
of internal environment we have created inside our bodies. No wonder
degenerative disease and premature aging are on the rise.
Sliding Down the pH Scale
At birth, most infants have a full supply of
alkaline reserves. This is reflected in a lymph pH of 7.4. As the
years go by, these reserves dwindle. And the system slowly becomes
more and more acid. This is primarily due to our super sized, fast
food/processed diet and our sedentary lifestyle. The staples of our
diet – protein, carbohydrates and processed foods leave acidic
residues that build up. Consider this – one cup of cola is so acidic
that you need to drink 32 cups of water to neutralize the impact.
With a diet that dumps acid residue into the system and the lack of
exercise to move the lymph through the body the result is a body
vulnerable to attack. Here’s how it works:
As the lymph becomes too acidic, fungi and
bacteria spontaneously develop and grow. When they reach the lymph
nodes they can clog the nodes, preventing proper function. As the
accumulation of waste piles up in the lymph, a semi-opaque web of
dark matter begins to form. At this point, not only is the lymph
acidic, oxygen depleted and growing microorganisms, it also flows
poorly. Unlike the heart, the lymph does not have a pumping
mechanism that can force it to flow. It relies on bodily movements
to advance the lymph in the Lymphatic System. As waste
accumulates, the lymph becomes stagnant and the growing
microorganisms are dumped into the blood stream, compromising our
immune system. We become susceptible to external microbes and
viruses and find ourselves “catching” every “bug” that floats by.
With an acidic system and our immune system compromised we are also
at risk of developing a degenerative disease.
Scary stuff, indeed. MMP Primary and Trace
Minerals with the accompanying nutrients were designed to restore
the lymph to its naturally alkaline state.
The Acid-alkaline Residue of Foods After
Digestion
It is an easy matter to measure the pH of foods
before eating it, either with pH strips or with a pH meter. However,
once digested, foods do not always have the same pH. A healthy
stomach digests food by first decomposing the food with the
digestive enzymes. Then the stomach secretes a strong hydrochloric
acid that continues to decompose the foods. After approximately 45
minutes, the food passes into the small intestine and there, an
amount of bile is injected into the food by the gall bladder. This
bile is strongly alkaline to neutralize the stomach acids. Next, the
food travels slowly through the small intestine and various
nutrients are extracted from the food and introduced into the blood
stream. From there, the nutrients go into the cells and are
processed to supply energy and building materials for repairs to the
body. Over time, the cells release the residue of the consumed
nutrients and this residue re-enters the blood stream. It is the pH
of this residue that is the focus of the MMP regimen.
From the time the food grows, either as
vegetable or animal, to the time its residue is released by our
cells into the blood stream, the pH can fluctuate considerably.
Generally, the fresher the food, the more alkaline it is, and it
becomes acid as it ages. Beef is aged for several days before
consumption and is the most acid food that we eat. By comparison,
chicken can be eaten fresh and often has an alkaline residue
depending on how the chicken was raised and how it is prepared.
Organically raised chicken that haven’t been subjected to external
stresses such as caging, generally have a more alkaline residue than
mass produced chicken that are loaded with antibiotics.
Fermented foods, however, should not be
considered as being aged, because they contain live bacteria that
are continuously changing the structure of such foods during
fermentation. As it happens, fermented foods will usually test very
acid before eating but after processing by the cells will have a
residue that is only weakly acid or even alkaline. This is the basis
of the macro-biotic diet that promotes eating living foods of all
kinds. Live foods usually have an alkaline residue, while the same
foods after sitting for weeks in the vegetable bins of chain stores
have a greater tendency to have an acid residue. The important point
is: the more alkaline (or less acid) a food is, the more sensitive
it is to aging. Therefore for maximum benefit it is best to consume
fresh alkaline foods. The most accurate list of acid-alkaline
residues of foods can be found in the book “The pH Miracle” by R.O.
Young and S.R. Young.
Of course, our modern diet and lifestyle
creates quite a challenge to consume fresh alkaline foods. Thus we
see the national adult average lymph pH of 6.2. By Restoring Nature
with MMP SOLUTIONS, you will be able to counter this dangerous trend
and reestablish your alkaline balance (even if you don’t change your
diet).
The MMP Solution
Our bodies are designed to absorb the minerals
we need from the food we eat. Unfortunately, due to environmental
pollutants and soil that is nutrient deficient this has become a
huge challenge. Even if one is very strict and diligent about
changing one’s diet and eating only high quality organic foods, you
would have to eat enormous amounts in order to get sufficient
minerals to support a slightly alkaline environment. The secret to
re-alkalizing the lymph is mineral absorption. MMP is the SOLUTION!
One serving of MMP Primary & Trace Minerals provides more
Alkalizing potential than 4 pounds of high quality organic
vegetables.
MMP SOLUTIONS provides:
- The fundamental alkalizing agents of
calcium, magnesium, potassium and sodium as carbonates and
bicarbonates.
- Three times as much calcium as the most
popular Coral Calcium capsule supplements.
- The proper 2:1 ratio of Calcium :
Magnesium.
- Over 70 Trace minerals
- Digestive Aids
- Vitamin D which is essential for calcium
absorption
- Hydrochloric Acid - [HCl] is the only
acid that our bodies produce. It is an active ingredient of our
digestive system. Secondary to digestive enzymes HCl’s function
is to break down food in the stomach. It is the first line of
defense against various destructive microbes that enter the
stomach. Many people have insufficient amounts of HCl which
results in digestive problems such as acid reflux and poor
absorption. Also, after the age of 40, HCl production begins to
decline. Lack of HCl combined with lack of properly balanced
minerals are the root cause of why the adult pH has declined to
an average of 6.2.
pH is afgeleid van het Latijnse potentia hydrogenii en betekent:
“werkzaamheid van de waterstof”.
Supplementing with minerals is
a stronger way to balance body acidity. A study
comparing calcium citrate and calcium carbonate
supplementation in postmenopausal women found that
calcium citrate decreased markers of bone breakdown both
in blood and urine, whereas calcium carbonate did not.
Otherwise, their performance was similar in improving
bone health. Sodium bicarbonate has been studied
extensively with mixed results.
Potassium citrate has shown
positive results. In one study, women with osteoporosis
given potassium citrate had increased bone density
significantly after a year- something very difficult to
achieve! It's important to follow the recommended doses
on labels because it's possible to get too much
potassium. If calcium is a concern because of kidney
stones, potassium citrate is a great alternative.
Minerals reduce acidity and give
your body's buffering systems a break. Systemic
alkalization has been shown to help with osteoporosis,
asthma symptoms, brain damage after stroke, preventing
kidney stones, cancer , and other conditions. Much more
research needs to be done.
Optimale pH waarde
- Bloed 7,35 - 7,45 (ideaal 7,41)
- Speeksel 7,20
- Cel 7,1
- Maag 1,35 - 3,50
- Urine 6,8 - 7,2
- Ontlasting 6,00 - 6,80
Al onze cellen baden in het extracellulaire
vocht dat net zoals het bloed licht basisch is (pH 7,35-7,45). De
uiterste pH-waardes waarbinnen nog leven mogelijk is liggen voor het
bloed en het extracellulaire vocht tussen 6,8 en 7,8. Te lage
pH-waardes (zuur) leiden sneller tot levensbedreigende situaties dan
te hoge waardes (basisch). Zo ontdekte dr. Berthold Kern dat een
verlaagde pH waarde (meer zuur) tot een verdikking van het bloed
leidde
Oorzaken van verzuring
- slechte voeding
- overmatig alcohol- en suikergebruik
- slechte eetgewoonten
- stressbelasting
- milieu invloeden
- verminderde functie van lever, nieren of
longen
- weinig beweging
- roken
- crash diëten
- overmatige sportactiviteiten
- veroudering
Het lichaam gebruikt pH buffers in het bloed
om zich te weer te stellen tegen te snelle
grote veranderingen in het zuurgraadniveau.
De meest belangrijke pH buffer in het bloed
is bicarbonaat. Bicarbonaat is een basische
stof en moet in het bloed in evenwicht zijn
met koolzuur. Als er meer zure stoffen het
bloed binnenstromen wordt er meer
bicarbonaat geproduceerd. Als er meer
basische stoffen de bloedstroom bereiken
wordt er meer koolzuur aangemaakt. In beide
gevallen wordt het effect op de pH
geminimaliseerd. Ook kan het lichaam
mineralen gebruiken om het bloed te
alkaliseren. Zoals men landbouwkalk gebruikt
om verzuurde grond weer alkalisch te maken,
zo gaat ons lichaam calcium, magnesium,
ijzer en andere mineralen roven om het bloed
te alkaliseren.
Ruwweg kan onze voeding onderverdeeld worden
in twee groepen:
1. Waterrijke voedingsmiddelen.
Deze zijn meestal volumineus, rijk aan
vitamines, mineralen en fytonutrienten en ze
bevatten weinig calorieën. Over het algemeen
hebben deze voedingsstoffen een
basen-overschot. Voorbeelden zijn: fruit,
groente, thee en melk.
2.
Geconcentreerde voedingsmiddelen.
Deze zijn vast van structuur, rijk aan vet,
eiwit en calorieën. Ze hebben over het
algemeen een zuren-overschot. Voorbeelden:
vlees, vis, ei, kaas, peulvruchten, noten, zaden
en granen. Suiker, koffie en alcohol zijn
uitzonderingen op de regel en zijn
zuurvormend.
bloem, bonen, erwten en vetten
| Acidity-in the body rising foods |
Score* |
| Fish |
14.6 |
| Meat |
12.4 |
| Poultry |
7.8 |
| Eggs |
7.3 |
| Shellfish |
7.3 |
| Cheese |
3.3 |
| Milk |
1.3 |
| Cereal Grains |
1.1 |
| Neutral foods |
Score* |
| Beans |
-0.4 |
| Base-producing foods |
Score* |
| Nuts |
-1.1 |
| Fresh fruit |
-5.2 |
| Potatoes |
-5.4 |
| Mushrooms |
-11.2 |
| Carrots |
-17.1 |
| Vegetable fruits(vruchtvormige
groenten) |
-17.5 |
| Leafy greens(blad groenten) |
-23.4 |
| Plant stalks (planten stam) |
-24.9 |
ph dranken:
Zeewater 8,5
Thee, naturel 7,1
Zuiver water 7,0
Melk, halfvol 6,8
Kruidenthee <6,0
Karnemelk 4,4
Bier 4,3
Yoghurt (drank) 3,8
Sportdrank 3,4
Rode/witte wijn 3,4
Kinder-Cola 3,3
7up 3,2
Sinaasappelsap 3,2
Limonadesiroop 3,0
Azijn 3,0
Cassis 3,0
Cola Light 2,9
Appelsap 2,8
Cola 2,7
Citroensap 2,0
Maagzuur 2,0
ALKALIZING MINERALS
Cesium: pH 14
Potassium: pH 14
Sodium: pH 14
Calcium: pH 12
Magnesium: pH 9
Rauwe groente sap ph 8.9
|
FOOD CATEGORY |
High Acid |
Acid |
Low Acid |
Low Alkaline |
Alkaline |
High Alkaline |
|
BEANS,
VEGETABLES, LEGUMES |
Pickled
Vegetables |
Pinto Beans,
Navy Beans |
Sweet Potato,
Cooked Spinach, Kidney Beans |
Squash,
Asparagus, Rhubarb, Fresh Corn, Mushrooms, Onions, Cabbage,
Peas, Cauliflower, Turnip, Beetroot, Potato, Olives,
Soybeans, Tofu |
Carrots, Green
Beans, Lima Beans, Beets, Lettuce, Zucchini, Carob |
Vegetable
Juices, Parsley, Raw Spinach, Broccoli, Celery, Garlic,
Barley Grass |
|
FRUIT |
|
Canned Fruit |
Blueberries,
Cranberries, Bananas, Plums, Processed Fruit Juices |
Coconut, Sour
Cherries, Tomatos, Oranges, Cherries, Pineapple, Peaches,
Avocados, Grapefruit, Mangoes, Strawberries, Papayas,
Lemons, Watermelon, Limes |
Dates,
Blackcurrant, Grapes, Papaya, Kiwi, Berries, Apples, Pears |
Dried Figs,
Raisins |
|
GRAINS, CEREALS |
|
White Rice,
White Bread, Pastries, Biscuits, Pasta |
Rye Bread, Whole
Grain Bread, Oats, Brown Rice |
Amaranth,
Lentils, Sweetcorn, Wild Rice, Quinoa, Millet, Buckwheat |
|
|
|
MEAT |
Beef, Pork,
Veal, Shellfish, Canned Tuna & Sardines |
Fish, Turkey,
Chicken, Lamb |
Liver, Oysters,
Organ Meat |
|
|
|
|
EGGS & DAIRY |
Parmasan,
Processed Cheese |
Eggs, Camembert,
Hard Cheese |
Whole Milk,
Butter, Yogurt, Cottage Cheese, Cream, Ice Cream |
Soy Cheese, Soy
Milk, Goat Milk, Goat Cheese, Buttermilk, Whey |
Breast Milk |
|
|
NUTS & SEEDS |
Peanuts, Walnuts |
Pecans, Cashews,
Pistachios |
Pumpkin, Sesame,
Sunflower Seeds |
Chestnuts,
Brazils, Coconut |
Hazelnuts,
Almonds |
|
|
OILS |
|
|
Corn Oil,
Sunflower Oil, Margarine, Lard |
Flax Seed Oil,
Olive Oil, Canola Oil |
|
|
|
BEVERAGES |
Tea (black),
Coffee, Beer, Liquor |
Wine, Soda/Pop |
Cocoa |
Ginger Tea |
Green Tea |
Herb Teas, Lemon
Water |
|
SWEETENERS,
CONDIMENTS |
Artificial
Sweeteners
|
Milk Chocolate,
Brown Sugar, Molasses, Jam, Ketchup, Mayonnaise, Mustard,
Vinegar |
White Sugar,
Processed Honey |
Raw Honey, Raw
Sugar |
Maple Syrup,
Rice Syrup |
Stevia |
video
Werking op het lichaam:
|
categorie:
|
zeer verzurend: |
verzurend: |
licht verzurend: |
licht alkalisch: |
alkalisch: |
zeer alkalisch: |
groenten, peul-
vruchten en wortels: |
ingelegde (in
zuur of pekel) groenten |
blikgroenten, diepvries-
groenten, champignons, zuurkool
|
gekookte groenten (alle soorten),
zoete aardappelen, kidney beans |
aardappels, paprika, sla, ui, prei, div.
kool, rabarber, aubergine, courgette, asperges, spruitjes,
erwten (vers), wortels, maïs (vers), mierikswortel,
koolrabi, koolraap, pompoen, pepers, zeewier |
tomaten, witlof, spinazie, sperciebonen,
snijbonen, rode biet, selderie, radijs, knoflook,
div. kruiden, alfalfa, gember |
komkommer, boerenkool, broccoli,
groentesap, kiemen, grassen |
| fruit: |
|
banaan (rijp), ananas, rozebottels,
granaatappel |
aardbeien, appel, peer, grapefruit,
sinaasappel, man-
darijn, pruimen, nectarine, mango, abrikoos, perzik, bessen,
meloen, cranberry, druiven, acai vrucht, papaya, zoete
kersen, dadels, frambozen |
vijgen,
citroen, limoen, watermeloen, banaan (onrijp), zure kersen,
kokosnoot (vers) |
avocado |
|
brood,
granen
en rijst: |
gebak, pasta |
tarwe, bruine rijst, tarwepitmeel,
witbrood, mais tortillas, haver, zuurdesembrood,
witte rijst, bruine rijst, cornflakes |
gist, gerst, basmati rijst, couscous,
haver, rogge, volkomen brood, witmeel cracker, tempeh
|
tofu, soja meel/bloem, amarant, linzen,
boekweit, spelt, wilde rijst
|
soja granulaat, witte bonen, lima bonen,
soja bonen |
soja noten |
| noten
en zaden: |
|
pinda's, pindakaas,
pistache noten
|
hazelnoten, paranoten, macadamia noten,
walnoten, cashews, lijnzaad, pompoenpitten, zonnebloempitten |
pijnboompitten, sesamzaad, karwijzaad,
kastanjes |
amandelen |
|
|
zuivel: |
kaas, gehomo-
geniseerde melk, ijs |
kwark, eieren, kaas, melk
(gepasteuriseerd) |
gehomogeniseerde melk, (slag)room,
yoghurt, melk (niet gepasteuriseerd), boter, rijstmelk,
sojamelk,
cottage cheese
|
karnemelk, geitemelk, geitekaas, wei |
borstvoeding |
|
|
dranken: |
koffie, thee, bier, frisdrank,
vruchtensap (gezoet), sterke drank |
spa rood, wijn |
kokosmelk, vruchtensap (ongezoet),
surrogaatkoffie |
gedisilleerd water, mineraalwater,
bronwater, kokosnoot water |
groene thee, rooibosthee |
citroenwater, kruidenthee |
| oliën: |
|
margarine |
boter, maïsolie, zonnebloemolie
|
olijfolie, lijnzaadolie, visolie,
kokosolie, sesamolie |
|
|
vlees
en vis: |
varkensvlees, rundvlees, kalfsvlees,
vis in blik |
oceaanvis, kip, kalkoen, lam,
schaaldieren |
zoetwatervis, orgaanvlees,
hert |
|
|
|
| zoet: |
zoetstoffen |
chocola,
melasse, stroop,
witte suiker,
bruine suiker, rietsuiker, bietsuiker,
xylitol |
bewerkte honing, rijst siroop, gerstemout
siroop, melksuiker, fructose, suikerrietsap, ahornsiroop,
agave diksap |
ruwe honing |
|
stevia |
|
diversen: |
sojasaus, azijn |
ketchup, mayonaise, mosterd, miso,
blikvoedsel, magnetronvoedsel |
appelwijnazijn, hummus, popcorn
|
Royal Jelly, bijenpollen |
zuiveringszout |
|
Acid-Alkali balance
From
DoctorMyhill
Maintaining the correct
acidity/alkalinity (or pH) of the blood is an
essential part of good health. Acidity and
alkalinity is determined by the concentration of
hydrogen ions - the lower the pH, the greater the
acidity and the greater the concentration of
hydrogen ions. It is important to realise the pH
scale is a logarithmic one. This means that the
difference between a pH of 7 and 4 means a thousand
fold increase in hydrogen ions. Such a shift would
have a massive effect on biochemical processes, most
of which are exquisitely sensitive to pH changes.
For normal metabolism, the pH of the blood is
tightly controlled by the lungs and the kidneys. In
the short term the lungs compensate where there is a
tendency to acidosis by slowing breathing so
retaining carbon dioxide and increasing bicarbonate,
and with that pH. In the medium term the kidneys
compensate - where there is acidosis, we pee out
acid.
This works fine when we have
enough acid or bicarbonate to play with. We run into
problems when we don't. Where there is poor
mitochondrial function, we slip into anaerobic
metabolism and produce lactic acid. This chronic
overproduction puts us into a permanently acidic
state. This means that any person with a tendency to
fatigue and anaerobic metabolism is likely to be
chronically acidotic. We try to correct this by
peeing out acid, but there is only so much we can
do! The possible effects of being acidic are:
An acidic body means we cannot
release glucose from the liver, nor can we make use
of sugar in blood and muscle (glycolysis is
inhibited). So mitochondria are further starved of
energy and the sufferer craves carbs, feeling
ghastly when he does not eat.
- Muscles contract less
strongly (see below)
- Acid urine strips out
minerals so we lose minerals too easily.
Acidic urine is a risk factor for osteoporosis.
- Plasma potassium
levels may rise.
Hyperventilation will worsen
any tendency to acidosis because it washes out
carbon dioxide, and therefore bicarbonate, from the
blood.
Muscles and acidity
I suspect there is another
effect on muscles. To understand this, think how
muscles work. There are two important protein
components, namely actin and myosin. They interact
like little men rowing a boat. The actin oars are
dipped in the myosin water and pull, so shortening
the muscle fibre. The oars are lifted out and take
another bite of water so the muscle filament is
ratcheted shorter. This process depends on the oars
being alternately sticky and then letting go. This
is depended on electrical forces. One moment there
is attraction and stickiness, next repulsion to let
go. These electrical forces are controlled by
electrons and protons, i.e. pH is vital! If the pH
is wrong, the oars are too sticky, do not let go of
the myosin and there is muscle damage. I suspect
this acidic tendency clinically is associated with
sore muscles, muscle cramps, spasms, tics and
restless legs.
Once started on magnesium
carbonate, many people comment that their early
morning stiff muscles are much improved!
Calcium and acidity
One of the biochemical
problems that John McLaren-Howard has identified is
a tendency for calcium to build up inside cells. The
cells try to tuck it out the way by sticking it on
to calcium containing proteins, such as calmodulin,
calcium-actin or CaATPase. This is OK in the short
term, but eventually these mechanisms become
saturated, free ionised calcium rises and inhibits
many of the mechanisms for energy production in the
cell. This calcium is not responsive to magnesium
administration, so what to do about it? We honestly
do not know! BUT calcium and hydrogen ions are
intimately related and the optimist in me is hoping
that an alkaline environment will help correct the
biochemical abnormalities. Watch this space!
Diagnosis
Easy and cheap. You simply
measure urine pH with litmus paper. The idea is to
get the pH between 6.5 and 7.0. Water has a neutral
pH of 7.0. Adjust the body's pH with judicious doses
of magnesium bicarbonate starting with 1-2 grams at
night, but see below! You do not want to
upset normal stomach acidity at the wrong time!
Acid and alkali in the gut
This is a vital part of
sterilising the gut, providing the correct pH for
digestion and absorption of food and minerals. We
need an acid stomach (pH 4 or below) to kill off the
acid sensitive bugs. This acidity also digests
protein and controls the emptying of the stomach.
Food remains in the stomach for 1-2 hours, then
empties into the duodenum. Here we need an alkali
environment (pH 8, i.e. a 10,000 fold decrease in
hydrogen ions) to kill the alkali sensitive bugs,
and allow pancreatic enzymes and bile salts to work
to digest fats, carbohydrates and some proteins.
Normally, the liver produces this bicarbonate but
can only do so if it has the raw materials to play
with.
Thus by manipulating the pH in
the gut we protect ourselves from infections -
something which many CFSs are not good at! Many are
helped by taking acid with meals, such as ascorbic
acid or betaine hydrochloride. We can help the
body further by taking magnesium carbonate to
neutralise this acid 1-2 hours after eating food.
It is important not to take the magnesium
bicarbonate with food or the gut function will be
upset. You can check that you are somewhere
near by measuring urinary pH. Do not overdose with
magnesium carbonate or you will run into problems of
being too alkali. You do not have to be too accurate
as the body is very good at compensating so long as
it has the basic raw materials to do so.
A traditional remedy is
sodium bicarbonate. The problem is this produces a
sodium load which, with Western diets, we are
already overloaded with. Magnesium carbonate is a
good option because magnesium deficiency is common,
and magnesium is all too easily excreted. Often
people report improved bowel function as a result of
the additional magnesium.
Alkaline Mineral Supplementation Decreases Pain in
Rheumatoid Arthritis
Patients: A Pilot Study
Regina Maria Cseuz1, Istvan Barna2, Tamas Bender3
and Jürgen Vormann*,4
1Revita Klinik, Budapest, Hungary; 2Institute of
Experimental Medicine of the Hungarian Academy of Sciences,
Budapest, Hungary; 3Hospital Brothers of St. John of
God, Budapest, Hungary, 4Institute for Prevention and Nutrition,
Ismaning, Germany
Abstract: The aim of this pilot study was to
investigate the efficacy of an alkaline mineral supplement as a
means of suppressing
disease activity in rheumatoid arthritis (RA)
patients, and to check whether any change occurs in the circulating
beta-endorphin concentration. Thirty-seven patients
with moderately active RA of at least two years duration, who were
receiving stable pharmacological treatment,
participated in a 12-week study. All patients were randomly
allocated to a
supplemented group (30g of an alkaline mineral
supplement daily) or to an unsupplemented group. Their usual diet
and
medication was maintained. Disease activity, pain,
and health-associated status were recorded (DAS 28 - Disease
Activity
Score 28, VAS - visual analogue scale for pain, HAQ
- Health Assessment Questionnaire). Plasma immunoreactive endorphin
(ir-EP) was measured in the study groups and also in
healthy subjects. DAS 28 and VAS decreased in the supplemented
group, whereas there was no change in these
parameters during the trial in the control group. The functions
(HAQ) of the supplemented patients improved. The
ir-EP levels increased in both groups but to a higher degree in the
supplemented group. During the trial, medication (NSAIDs
and steroids) could be reduced in the supplemented group
only. Conclusion: This study suggests that an
alkaline supplement may improve function and pain in rheumatoid
arthritis
and may represent an easy and safe addition to the
usual treatment of RA patients.
Keywords: Pain, rheumatoid arthritis, acid-base balance,
beta-endorphin.
INTRODUCTION
A large body of epidemiological and experimental
studies
has demonstrated that nutrition has an important
impact
on the occurrence and severity of various chronic
diseases
[1]. The level of disease-associated pain may also
be dietrelated.
For example, patients with rheumatoid arthritis (RA)
frequently experience a positive effect of a change
in diet on
the activity of their disease. The hypothesis of our
present
study was that patients with RA, consuming an
ordinary
Western diet as most of the population of the
world's developed
countries, develop a diet-induced low-grade systemic
metabolic acidosis [2]. There is strong evidence
that a diet
rich in fruit and vegetables acts protectively
against a wide
variety of human diseases. However, such a diet
usually also
supplies excess alkalinity, and part of its
beneficial effects
might be associated with a reduction of the chronic
acid load
[3]. The chronic inflammatory process in RA patients
leads
to a local increase in acidity; the pH in synovial
fluids from
patients with RA is significantly lower than that in
patients
with osteoarthritis or controls [4]. This change in
local acidity
might aggravate pain symptoms, especially in
connective
tissues. Therefore, alkaline supplementation might
lead to an
improvement of the clinical outcome in RA patients.
In patients
with chronic low back pain, alkaline supplementa-
*Address correspondence to this author at the
Institute for Prevention and
Nutrition, Adalperostr. 37, D-85737 Ismaning,
Germany; Tel: +49 (0)89
55267989; Fax: +49 (0)89 55267990; E-mail: vormann@ipev.de
tion significantly reduces pain and disability [5].
Our own
observations of some RA patients also suggest the
positive
effect of a complementary treatment with alkalines.
We have
therefore conducted a pilot study to investigate, in
more detail,
the effects of an alkaline supplement on pain
symptoms
in patients with RA. In addition to subjective
indicators of
pain, disability, and quality of life, the change of
the concentration
of beta-endorphin (ir-EP) has been determined in the
plasma of patients as a more objective parameter of
pain
problems. Significantly lower ir-EP levels have been
reported
in RA patients than in controls, and an inverse
correlation
has been found between the rheumatoid disease
activity
score and plasma ir-EP concentration [6].
MATERIALS AND METHODS
Patients and Study Design
Prior to commencing the study, approval by the local
ethical committee (Scientific Committee of St John’s
Hospital,
Budapest) was obtained, and the ethical principles
of the
Helsinki Declaration were followed. All patients
were informed
orally and in writing about the study design and the
underlying hypothesis and of the participant’s right
to withdraw
at any time. The study design was a single-center
randomized
parallel trial over a period of three months.
Patients
Out of 76 outpatient candidates who were screened
for
the trial and were willing to participate, 37
patients fulfilled
all the inclusion criteria according to Table 1.
These patients
were randomly selected into a supplemented group or
an
unsupplemented control group. Baseline
characteristics of
patients in both groups are shown in Table 2.
Supplementation
After a 4-week wash-out period (other supplements),
patients in the supplemented group started to take,
on a twice
daily basis, 30 g (2 x 15 g) of a lactose-based
alkaline multimineral
supplement (Basica Vital®, Protina Pharmaceuticals,
Germany) for a 12-week period in addition to their
usual medication. The mineral composition was as
follows
(mg/daily dose): Ca (400), K (250), Na (250), Mg
(100), Fe
(5), Cu (1) all as citrates, Zn (5) as gluconate, I
(0.1) as potassium
iodide, Mo (0.08) as sodium molybdate, Cr (0.06) as
chromium chloride, Se (0.03) as sodium selenite. The
alkaline
mineral supplement was taken twice daily in the form
of
a powder mixed in one of the following: soup,
yoghurt, tea,
or cereal. A suitable inert placebo in a similar
daily dose was
not available, and the use of sugar as a placebo seemed not
to be appropriate. Therefore, a placebo was omitted
in this
pilot trial. During the trial, patients were not
allowed to take
any dietary supplements except for the alkaline
mineral supplementation
in the supplemented group. The individual dose
of non-steroidal anti-inflammatory drugs (NSAID)
could be
adjusted but had to be recorded.
Determinations and Measurements
All patients were evaluated by the same investigator
in
accordance with a written protocol that included
medical
history, ACR criteria [7], complete evaluation,
articular
evaluation, and extra articular evaluation of RA
(history of
rheumatoid nodules, Reynard’s phenomenon, or
pulmonary,
cardiac, dermal, ocular, and nervous system
involvement).
Disease activity was assessed by determination of
the number
of swollen joints, the score of tender and swollen
joints,
and the duration of morning stiffness (in minutes).
A composite
disease activity score (DAS 28) [8], a physical
function
index Health Assessment Questionnaire (HAQ) [9],
Creactive
protein (CRP), and rheumatoid factor were measured
at baseline and 4, 8, and 12 weeks after starting
the
trial. DAS28 is a composite disease activity index
and also a
response index with good discriminatory validity. It
includes
28 joint counts for tenderness (tender joint count)
and swelling
(swollen joint count), the erythrocyte sedimentation
rate
(ESR), and the patient's global assessment of
disease activity
on a horizontal visual analog scale (patient global
VAS, 0-
100mm). As a parameter connected to pain, the level
of ir-
EP was determined in blood samples of both patient
groups
and from healthy subjects (6 females, 6 males; mean
age: 45
years). Blood samples were collected into
K2-EDTAcontaining
plastic tubes and then centrifuged, after which
plasma aliquots were stored at –20 °C until assayed.
Details
of the EP radioimmune assay (RIA) including the
percental
cross-reaction data were as described earlier [10].
In short,
synthetic human EP (Sigma) was used both for the
standard
and 125I-labeled tracer, and a second antibody was
used to
separate the bound and free fractions.
Compliance
Compliance of supplemented patients was monitored by
the weekly determination and recording of the pH of
the first
morning urine with pH paper strips by the patients
themselves.
Supplementation induced a significant increase in
urinary pH by at least one pH unit after one week in
all supplemented
patients and remained high throughout the
supplementation
period thus indicating adherence to the supplement.
Statistical Methods
Determined parameters were normally distributed and
variations were compared between time 0 and 4, 8,
and 12
weeks, respectively, and between the supplemented
and unsupplemented
groups by using Student’s t-test. Frequencies
of reduction of medication were compared between
groups
by means of the Fisher exact test. All reported P
values are
2-sided.
RESULTS
A total of 37 patients were enrolled of whom 19 were
randomly allocated to the supplemented group and 18
to the
unsupplemented control group. In one control patient, an
intra-articular injection with triamcinolone
hexacetonide was
reported what expectedly influenced the disease
acitivity,
and this patient was excluded from the study. Hence,
19 supplemented
and 17 control patients completed the trial. At the
start of the experiment, the two groups were equal
in all respects,
except for disease activity score (DAS28). At
baseline,
the control patients showed a score of 4.5 (range:
2.8-
6.0) versus the supplemented group with a score of
5.2
(range: 3.6-6.9); this difference is statistically
significant (ttest).
At the end of the observation period, the
supplemented
group, in which members had started with
significantly
higher disease activity score, showed significantly
lower
DAS28 compared with control patients (Fig. 1).
DAS28 decreased
in the supplemented group, whereas there was no
significant change in disease activity score during
the trial in
the control patients. There were also significant
differences
between supplemented and unsupplemented groups at 4,
8,
and 12 weeks. The level of pain (according to the
patient's
visual analog scale (VAS)) decreased to a
considerable extent
in the supplemented group (Fig. 2). In the
control patients,
the pain increased between week 0 and week 4. Be-
Fig. (1). DAS28 in supplemented (first column)
and unsupplemented
(second column) RA patients at 0, 4, 8, and 12
weeks. Significant
difference in comparisons with time 0 of the
respective
group; a: p = 0.049; b: p = 0.011, c: p = 0.004.
Significant differences
between groups; A: p = 0.006; B: p = 0.016, C: p =
0.028;
mean ± SEM.
Fig. (2). Pain level according to a visual
analog scale in supplemented
(first column) and unsupplemented (second column) RA
patients at 0, 4, 8, and 12 weeks. Significant
difference in comparisons
with time 0 of the respective group; a: p = 0.045;
b: p = 0.004,
c: p = 0.048. Significant differences between
groups; A: p = 0.003;
B: p = 0.001, C: p = 0.037; mean ± SEM.
tween groups, significant differences were detected
after 4,
8, and 12 weeks. HAQ results showed a significant
improvement
in supplemented patients by the end of the trial,
whereas no change was seen in the control patients
(Fig. 3).
At the end of the trial, the difference between
groups also
became significant.
Fig. (3). Physical function index (HAQ) in
supplemented (first
column) and unsupplemented (second column) RA
patients at 0, 4,
8, and 12 weeks. Significant difference in
comparisons with time 0
of the respective group; a: p = 0.009. Significant
differences between
groups; A: p = 0.049; mean ± SEM.
ESR, CRP, and the level of rheumatoid factor showed
no
significant change during the trial in either of the
groups (not
shown).
In healthy subjects, the plasma ir-EP levels were
significantly
higher than in RA patients: (plasma ir-EP in fmol/ml,
mean ± SEM) healthy subjects, 12.6 ± 3.9 (n = 12);
RA patients,
4.1 ± 0.5 (n = 37). Plasma ir-EP levels
significantly
increased in the supplemented and control group;
however,
the increase in the supplemented group occurred
earlier and
was higher than in the control patients (Fig. 4);
at the end of
the supplementation period, there was also a
significant difference
between both groups.
Fig. (4). Plasma endorphin concentration in
supplemented (first
column) and unsupplemented (second column) RA
patients at 0, 4,
8, and 12 weeks. Significant difference in
comparison with time 0
of the respective group; a: p = 0.016; b: p = 0.018,
c: p = 0.045.
Significant differences between groups; A: p =
0.043; mean ± SEM.
At the end of the study, the medication of 6 out of
19
supplemented patients was reduced: in 3 patients,
the daily
steroid dose was decreased by 2-4 mg, and three other pa
patients
no longer needed to take NSAIDs. In the control
group, one patient had to be put on medication
because of
hypertension during the trial, and one patient's
steroid dosage
had to be increased, in the other patients
medication was
unchanged. The reduction in medication in the
supplemented
compared with the control group was statistically
significant
according to the Fisher´s exact test (p=0.014).
DISCUSSION
The cause of RA is still unknown, but it is likely
to involve
both genetic susceptibility and environmental
factors
such as diet [11]. The role of nutrition should be
clarified
with respect to two fundamental aspects: 1) Does it
have any
effect in the clinical expression of the disease or
in susceptibility
to RA? 2) Could any diet or nutrient supplementation
play a role in the management of RA by alleviating
symptoms
such as pain, by decreasing the progression of the
disease,
or by reducing the reliance on or combating the
sideeffects
of NSAIDs ? [12].
Case-controlled studies indicate that the lifelong
consumption
of fish, olive oil, and cooked vegetables may have
protective effects on the development or severity of
RA [13,
14]. Patients with RA have been reported to consume
too
much total fat and too little polyunsaturated folic
acid
(PUFA) and fibre [15]. The so-called Western diet
(which is
also ingested by most of the population in Hungary)
is well
known to lead to the development of latent metabolic
acidosis
[16]. Compensation of this acidosis is possible by
increasing
the intake of organic mineral salts either from the
diet (increased intake of vegetables and fruits) or
from supplements.
The main alkaline substances in our diet are
citrates;
a useful supplement therefore should contain a
mixture
of various citrate salts of sodium, potassium,
calcium, and
magnesium. The used supplement contains all these
salts,
together with trace elements and lactose, which
increases the
bioavailability of minerals. The used dose of the
supplement
provides a total of 45 mEq base per day. The usual
daily
surplus of acid in the Western diet is 60 mEq in an
elderly
population [17], and so a significant reduction in
acid load is
achieved with the supplementation. There is to date
no indication
that single constituents of the supplement alone
work
in improving the symptoms in RA patients.
Supplementation of the usual diet with alkaline
minerals
improved the DAS28 in this study. Of the
contributory factors
of DAS, the level of pain changed most remarkably in
the supplemented group; however, laboratory
parameters
indicating the degree of inflammation (ESR, CRP) did
not
change in either of the groups, indicating that the
severity of
the disease by itself was not influenced by the
supplementation.
One might argue that plasma parameters of acid-base
status (pH and bicarbonate values) should have been
determined
in this study; however, these parameters are
extremely
well buffered, and changes in these parameters are
much
smaller than the probable pH or buffer changes in
the interstitium
[18].
The reduced pain sensation can be explained by the
significant
elevation of plasma ir-EP levels following alkaline
supplementation. The exact physiological role of
circulating
ir-EP is still obscure. What is clear from
biochemical studies
is that ir-EP binds predominantly to the mu opioid
receptors
[19] that are present in several peripheral tissues including
immune cells [20, 21] and the synovial membrane
[22]. Sporadic
experimental data suggest that peripheral ir-EP and
its
opioid receptor system play a role in the physio-pathology
of
local inflammatory processes. The above experimental
results
and the reported negative correlation between RA
activity
and plasma ir-EP levels [23], together with the
general
opinion that relative ir-EP deficiency may play a
part in the
manifestation of autoimmune diseases [24, 25], all
suggest a
causality between the circulating ir-EP levels and
the arthritis-
induced pain.
In addition to a pain-reducing direct effect of
endorphins,
an alternative explanation might be the more
alkaline environment
in the local surrounding of the joints, as pain
receptors
are sensitive to small pH changes. Significant
changes in
pH have been shown to occur in the interstitium
without detectable
changes in blood pH [18].
The finding that 6 out of 19 patients taking an
alkaline
supplement could reduce their daily steroid or NSAID
dosage
also supports the view that a reduction in latent
metabolic
acidosis has a positive effect on pain sensation. As
the
chronic need for pain medication is connected to
potential
side-effects, it is of great importance to find safe
adjuvant
therapies for these patients, such as
supplementation with
alkaline minerals, even though the supplementation
does not
influence the severity of the disease itself.
The limitations of this study include its small
sample size
and the lack of an active control group. However,
the results
of this pilot trial should encourage further
randomized placebo-
controlled studies to investigate the effects of
alkali
therapy.
CONCLUSIONS
Studies of the effects of dietary habits and
nutrient supplementation
on RA are, to quote Ollier et al. [26],
"hampered
by the inherent variability in the clinical course
of the
disease and the wide spectrum of clinical
phenotypes." Patients
frequently self-prescribe complementary medicines
including diet modifications. This leads to
considerable difficulties
in selecting an appropriate group of patients for
study. Improvement in symptoms may be dependent on
the
severity of the disease and on the underlying
inflammatory
status. An important finding of this study is the
significant
decrease in pain and DAS28 level and elevation in
plasma ir-
EP levels following several weeks of alkaline
supplementation.
Our study is the first to demonstrate the effect of
the
metabolic acid-base balance on plasma ir-EP levels.
The
results of our study suggest that an alkaline
supplement may
improve function and pain in rheumatoid arthritis
and represents
an easy and safe addition to the usual treatment of
RA
patients.
|